There are many sub-types of thyroid cancer. Papillary and follicular thyroid cancers account for 80-90% of them. They tend to grow slowly and if detected early, both can be treated successfully.
There are many sub-types of thyroid cancer. Papillary and follicular thyroid cancers account for 80-90% of them. They tend to grow slowly and if detected early, both can be treated successfully.
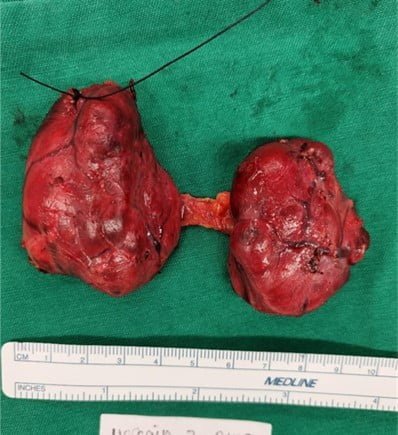
Thyroid cancer surgery remains the main treatment in most cases of thyroid cancer.
There are many sub-types of thyroid cancer. Papillary and follicular thyroid cancers account for 80-90% of them. They tend to grow slowly and if detected early, both can be treated successfully.
Thyroid cancer surgery remains the main treatment in most cases of thyroid cancer.